

 The Trump administration couldn’t abolish the Affordable Care Act (ACA), but it did make significant changes to it and work requirements for Medicaid likely to reduce the availability of coverage or discourage enrollment. So, after years of declining uninsured rates, the U.S. saw coverage gains stall--and for some groups, even drop. That’s a key takeaway from The Uninsured and the ACA: A Primer, a 2019 report from the Kaiser Family Foundation (KFF). It provides information on how insurance has changed under the ACA, how many people remain uninsured, who they are and why they lack health coverage. We’re taking a look at what this means for our clients--and how Altruis can help.
The Trump administration couldn’t abolish the Affordable Care Act (ACA), but it did make significant changes to it and work requirements for Medicaid likely to reduce the availability of coverage or discourage enrollment. So, after years of declining uninsured rates, the U.S. saw coverage gains stall--and for some groups, even drop. That’s a key takeaway from The Uninsured and the ACA: A Primer, a 2019 report from the Kaiser Family Foundation (KFF). It provides information on how insurance has changed under the ACA, how many people remain uninsured, who they are and why they lack health coverage. We’re taking a look at what this means for our clients--and how Altruis can help.
FQHCs and other safety-net clinics may soon take a financial hit. Changes in work requirements for Medicaid and the ACA are creating a new group of uninsured individuals. These newly uninsured are more likely to be poor, and most won’t have the resources to pay the bill. Clinicians, health centers and hospitals will be forced to write off those costs.
KFF’s The Uninsured and the ACA: A Primer, offers troubling, yet valuable, insights into the growing number of individuals without insurance. We’ve identified several and explore the implications for safety-net providers.
Work Requirements for Medicaid and the ACA evolve--or devolve
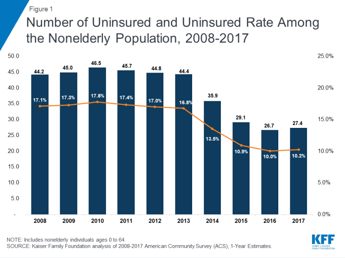
Millions of people enrolled in ACA coverage, and the uninsured rate dropped to an historic low by 2016. Coverage gains were particularly large among low-income adults in states that expanded Medicaid. There were still people who fell through the cracks, due to the 2012 Supreme Court decision upholding the law but striking down the Medicaid expansion requirement. But since 2017, the situation has become worse. The number of uninsured rose for the first time since ACA implementation--it’s now roughly 27.4 million, according to the KFF report.
- The reason: Ongoing efforts to alter the ACA or make Medicaid more restrictive have led people to drop or forgo coverage. Others are--or soon will be--ineligible based on new work requirements for Medicaid. Here are some of the most significant changes.
- No more individual mandate: As part of the December 2017 tax reform bill, Congress got rid of the individual mandate. The lack of a penalty could deter healthier people from enrolling in coverage. And that means higher rates: KFF’s analysis found that plans increased premiums to account for the loss of the individual mandate, and that will affect those already paying hefty premiums--those without subsidies and those with individual coverage outside the ACA marketplace. Moreover, eliminating the penalties for not having health insurance will result in anywhere from 2.8 to 13 million fewer Americans with coverage, the Commonwealth Fund estimates.
- New, less-regulated plans: In 2018, the Trump administration announced rules that will
 permit more loosely regulated plans. These plans--"short-term limited-duration” plans and association health plans--will be allowed to compete in the individual marketplace. Although they will provide a more affordable option for some, these plans are generally unavailable to people with pre-existing conditions, and they exclude coverage for certain services. Because these plans attract disproportionately healthy individuals, they will lead to increased premiums for ACA-compliant plans, according to a 2018 KFF report.
permit more loosely regulated plans. These plans--"short-term limited-duration” plans and association health plans--will be allowed to compete in the individual marketplace. Although they will provide a more affordable option for some, these plans are generally unavailable to people with pre-existing conditions, and they exclude coverage for certain services. Because these plans attract disproportionately healthy individuals, they will lead to increased premiums for ACA-compliant plans, according to a 2018 KFF report.
But it’s the changes to Medicaid that will likely have the greatest impact on safety-net providers.
Work Requirements for Medicaid under fire
CMS has for years approved certain eligibility- and enrollment-related provisions as part of Medicaid expansion waivers. Now, the Trump administration has approved new, much more draconian, restrictions. Interest in these waivers has “skyrocketed,” according to Modern Healthcare. This makes it harder for vulnerable patients to get insurance coverage--and for providers to be paid. In Arkansas, for instance, more than 18,000 people lost Medicaid in 2018 for failing to meet work or reporting requirements.
Here’s an overview.
- Work requirements for Medicaid: Perhaps most significant is the continued push for work requirements; Kentucky still plans to roll out Medicaid work requirements on April 1, 2019, and we expect other states to follow suit. The absurdity of it is that most people on Medicaid already work or are exempt (in school, have a disability or care for a child or an elderly relative). An earlier KFF study, released in June 2018, concluded that only 6 percent of non-exempt, able-bodied adults on Medicaid are not working. Many who do work, however, may be unable to meet the minimum-hours threshold because they hold jobs with irregular hours, warns the Center on Budget and Policy Priorities.
- Lockouts: Several waiver proposals include punitive “lockout” provisions, often used to enforce premium payment and work requirements. Other states have proposed locking out any beneficiary who misses the eligibility redetermination deadline or fails to report a “change in circumstance.” Handling all the paperwork is already a challenge: As Health Affairs points out, many lack the email and Internet access needed to file paperwork. Most Medicaid enrollees locked out of coverage will remain uninsured. Ultimately, we believe lockouts will create higher levels of uncompensated care.
- Retroactive coverage: In 2018,Florida won approval to eliminate retroactive eligibility, which gave patients 90 days of Medicaid coverage prior to their application date. Alaska, Iowa, Indiana, Kentucky, New Hampshire, Florida and Utah have had the waivers approved. Three states are pending: Arizona, New Mexico and Maine.
- Lifetime limits: The threat of lifetime limits on Medicaid continues to rear its head. Arizona and Kansas were headed in this direction, but Arizona withdrew its proposal, and CMS rejected Kansas’ request, according to McGuireWoods Consulting. Expect the issue to come up again.
- Immigration and public-charge rules: “Public charge” refers to someone considered dependent on the government for subsistence. An immigrant considered likely to become a public charge may be denied permanent-resident status. In October 2018, the Trump administration published a proposed rule that would allow officials to consider use of certain previously excluded programs, including Medicaid, in public-charge determinations. This will likely lead to lower Medicaid participation among legal immigrant families--even those with children who were born in the U.S. If these families do seek care, it will be self-pay. Similarly, changes in immigration policy have led immigrant families to turn away from Medicaid and CHIP, according to the KFF report.
Falling backward
These changes place a tremendous strain on patients, discouraging them from seeking the care they need. They also increase the pressure on safety-net providers, for several reasons. Individuals who delay seeking care become sicker; when they finally do seek care, it’s more likely to be in an emergency department. If they do visit a clinic, they probably are sicker and costlier to treat.
These changes also mean fewer patients are likely to have any form of insurance, leaving providers with a pile of AR that will have to be written off. We don’t know exactly what’s in that particular pile of AR, but Altruis can help identify who might actually be eligible for Medicaid or still had coverage at the time of the visit.
Many self-pay patients obtain Medicaid after their initial visit. A significant percentage of self-pay patients are eligible--or become eligible--for Medicaid coverage. Altruis analyzes self-pay encounters on a daily basis to identify when a patient has been qualified to receive coverage. The patient is then enrolled, and their eligibility is applied retroactively to cover the costs of previously provided care. We then bill Medicaid for the encounters and collect every dollar for this previously uncompensated care.
Our retroactive Medicaid solution creates new revenue streams by automating the process that identifies coverage and bills payors. That takes stress off clinicians and patients alike. However, keep in mind that several states plan to eliminate retroactive Medicaid payments. If you want to collect for previously uncompensated care, you need to act now, not later. Contact us today to find out about our RetroPay services.

